
Navigate the page:
What is Periodontal Disease?
What is the Cause of Periodontal Disease?
How do we treat gum disease?
Can I Get Sick Without Treatment?
This is the destruction of the tooth ligament.
Many people think teeth are held in by the bone and gum tissue, by a direct bone-to-root interface. The truth is that there is a soft tissue union 0.2mm in width between the bone and the tooth root called the periodontal ligament. It is made of collagen essentially. It is extremely narrow yet very complex.
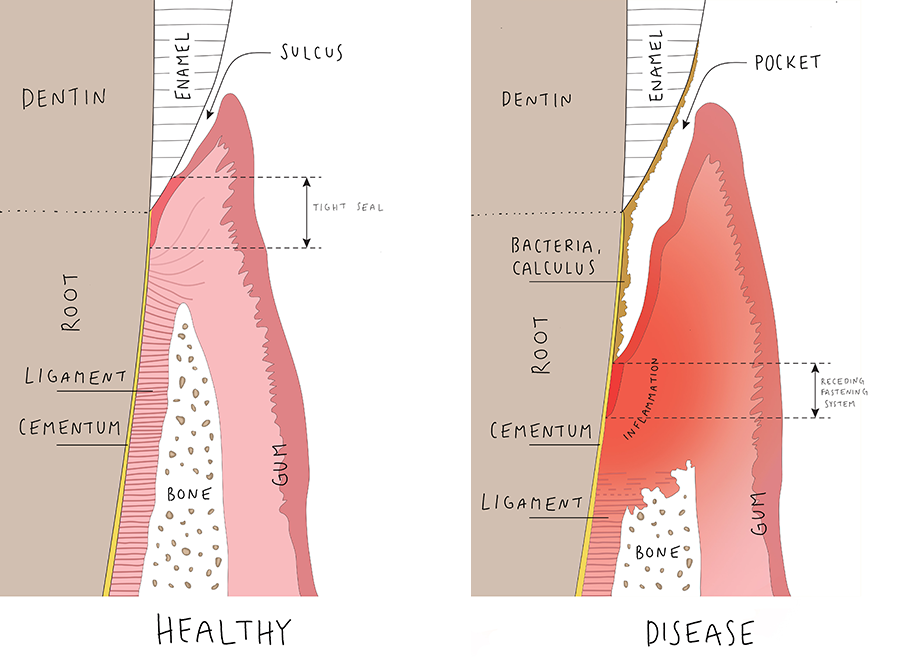
Think of this ligament as a Velcro fastener: it inserts on one side to the bone socket lining and on the other side it inserts in the outer layer of the root surface called the cementum.
This complex tissue allows the tooth to function under the load of chewing and absorb excess pressure from clenching and grinding. The ligament is also involved in tooth movement and aids in the eruption of the tooth. Above all, it anchors teeth into your jaw.
This finely-engineered fastening system works very well as long as it is kept isolated from the toxic environment of your mouth. Gums, when healthy, represent an effective barrier to a variety of insults to this deeper delicate tissue. They surround the teeth and provide a seal around them. In optimal condition of hygiene, there is a strong chemical bond between the gum and the enamel layer-not unlike the skin around your nails- that allows for the stability of tissues beyond this seal (bone, ligament, vessels).
It is dental plaque; that sticky, whitish film building up on your teeth when you don’t brush them meticulously twice a day.
Dental plaque is a biofilm: essentially, a slimy matrix produced by a variety of pathogenic bacterias in which they are embedded. It constantly forms on your teeth. Right after brushing, it rebuilds again, even if you do not eat anything. It is like Sisyphus’ boulder that forever rolls back down the hill on nearing the top! After a few days, plaque even begins to harden into a rough, porous material known as calculus.
If left undisturbed on your teeth, dental plaque initiates an inflammatory reaction that is, by definition, intended to defend the gingiva and the ligament against the bacterial challenge. However, it is ineffective in doing so because technically, plaque is located outside the body tissues and therefore cannot be drained by lymph or blood vessels. Over time, inflammation perpetuates itself and leads to tissue damage. This means the snugly fit of gum tissue around the neck of the tooth eventually breaks down and cannot any longer provide tissue integrity, nor defense against the invasion of bacterial products toward the tooth ligament. Slowly, the collagen fibers the periodontal ligament is made of begin to disintegrate.
The whole process soon causes the gum tissue to pull away from the tooth root, forming a space, or ‘pocket’, between the gum and tooth where calculus and plaque continues to accumulate, getting closer and closer to the bone beneath. At that point gums are red, swollen, bleed easily (spontaneously or on gentle exploration of the pocket with a periodontal probe), and may even suppurate. That inflamed gum tissue is the perfect venue for more bacteria and toxic material to hide. Consequently, the root surface now is like the hull of a boat covered with algae and shellfish.
If this situation is left to develop further, the ligament -this great “Velcro fastener” we mentioned above- will be dramatically reduced or lost. In those areas, the adjacent bone degenerates. It is no longer attached to the tooth and cannot provide any support.
In later stages, more supporting bone is destroyed and your teeth will shift, loosen, or fall out. These changes not only affect your ability to chew and speak. They also spoil your smile and your breath.
With proper hygiene, only the initial stage of the disease, referred to as gingivitis, is reversible. Unfortunately, once inflammation reaches the ligament, it cannot be reversed.
After thorough numbing of the area, this non-surgical procedure entails placing a fine ultrasonic tip and/or hand scraper between the tooth and gum (in pockets) to remove plaque and tartar below the gum line. Root planing is also performed in order to remove cementum and surface dentin that is embedded with unwanted microorganisms and toxins. The root of the tooth is literally smoothed. This, combined with excellent personal oral hygiene allows the gum tissue to heal and reattach to the tooth: 8 to 10 weeks later, the periodontal pockets are reduced or eliminated through the resolution of the inflammatory reaction.
It is very important that you comply with Dr Gaumet (or the hygienist) oral hygiene instructions during this phase.
After 8 weeks Dr Gaumet will evaluate the response of your gums to that therapy. If you still present with residual pockets, you might well be a good candidate for a second procedure. The issue with pockets is that, technically, they just cannot be kept clean with daily at-home oral hygiene, even the hygienist won’t be able to do a perfect cleansing. With inflammation-inducing material at the bottom of it, the potential for the recurrence of periodontal disease still remains high in susceptible individuals.
In essence, the goal of surgery is to eliminate pockets, and recreate a tooth environment that is more conducive to oral hygiene and maintenance care so that teeth can be kept for the long term. It facilitates home care, so to speak. Pockets vanish through re-attachment of the gingiva or the ligament onto the root surface.
The procedure entails numbing the area first with a local anesthetic. The gum tissue is gently pulled away from the tooth and a flap is raised, much like opening the flap of an envelope. This allows for direct access to the pocket environment: inner diseased tissue is removed, bacterial deposits can be scraped off and the tooth root cleaned and detoxified. Back tooth surfaces are very convoluted, with many nooks and crannies where bacteria and calculus can hide. Those areas can only be accessed surgically.
To complicate things further, inflammation by-products often erode the bone. It becomes jagged and uneven, and needs to be smoothed and reshaped with drills and hand tools. Bone is removed in some areas to restore its normal rise (between teeth) and fall. This will achieve great gum contour upon healing, more amenable to hygiene.
Bone grafting may also be necessary to fill in large defects. A bone graft usually originates from elsewhere in your jaw or it is purchased from a tissue bank. It looks like kosher salt and provides the scaffolding needed to regrow your damaged bone. Rarely, additional procedures may include use of growth factors which are proteins that stimulate the stem cells in the wounded area and facilitate healing.
Finally, the gums will be placed back over the remaining bone and retained around teeth with stitches.
To ensure long term health after your treatment, it’s critical to make sure it doesn’t come back. Even after treatment, whether surgical or non-surgical, gum disease patients are always at risk of the inflammatory reaction being triggered again in some area. That’s why patients with a history of gum disease will need regular periodontal maintenance at 3 month intervals to prevent the recurrence of the disease. Periodontal surgery is not a cure, but rather an adjunct to making long-term treatment outcomes more favorable.
Even with the most religious home brushing and flossing routine, it is nearly impossible to remove all deposits and bacteria in the hard to reach areas such as concavities and crannies of the roots. The maintenance visit consists of meticulous cleaning below the gum line, polishing of the teeth, home care education, and evaluation of the pocket depth.
Definitively yes!
For the past 10 years, we have been learning more about how periodontitis can affect your overall health. It is a new and exciting field of research.
Without treatment, you are at increased risks of developing atherosclerosis and heart disease, diabetes, Alzheimers, some cancers (esophagus, pancreas), respiratory disease, rheumatoid arthritis.
This chronic, painless, local inflammation appears to trigger a chain of events in your body by which too much inflammation-inducing chemicals are pumped out in your blood, such as the C-reactive protein(CRP). This may wreck havoc on your organs: many of the diseases that affect us as we age are now thought to be caused by, or worsened by, chronic inflammation.
For more information or to schedule a consultation, contact us today or call Dr. Gaumet’s office 41 21 323-7564.